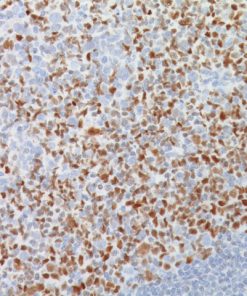
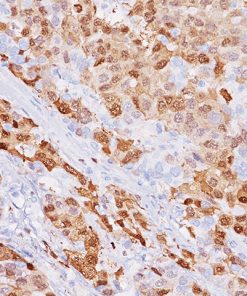
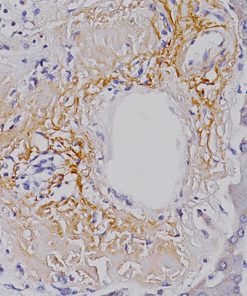
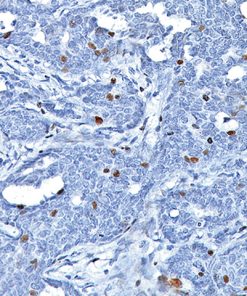
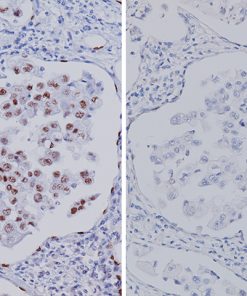
– Lung adenocarcinoma stained with TTF-1 [SPT24] / (R) – Lung adenocarcinoma stained with TTF-1 [8G7G3/1]")

TTF-1 [SPT24]
Price range: $270.00 through $1,022.00
Description
Product Description
Thyroid transcription factor-1 (TTF-1) is a 38 kDa member of the NKX2 family of homeodomain transcription factors. TTF-1 is mostly detected in primary lung adenocarcinomas and small cell carcinomas.1 No cytoplasmic staining in lung cancers has been observed with clone SPT24.2
Specifications
Specifications
| Intended Use | |
|---|---|
| Format | Concentrate, NeoPATH Pro, ONCORE Pro, Predilute, Q Series, UltraLine |
| Volume | |
| Source | |
| Clone | |
| Isotype | |
| Antigen | |
| Localization | |
| Positive Control |
Datasheets & SDS
| Download CE Marked IVD Datasheet |
| Download IVD Datasheet Without CE Mark |
| Download RUO Datasheet |
| Download SDS Sheet |
Browse more documents for this product (IFUs, datasheets, translations, SDS, and more).
References
1. Di Loreto C, et al. Immunocytochemical expression of tissue specific transcription factor-1 in lung carcinoma. J Clin Pathol. 1997 Jan; 50(1):30-2.
2. Tacha D, et al. A 6-antibody panel for the classification of lung adenocarcinoma versus squamous cell carcinoma. Appl Immunohistochem Mol Morphol. 2012 May; 20 (3):201-7.
3. Brown AF, et al. Tissue-preserving antibody cocktails to differentiate primary squamous cell carcinoma, adenocarcinoma, and small cell carcinoma of lung. Arch Pathol Lab Med. 2013 Sep; 137(9):1274-81.
4. Masai K, et al. Expression of squamous cell carcinoma markers and adenocarcinoma markers in primary pulmonary neuroendocrine carcinomas. Appl Immunohistochem Mol Morphol. 2013 Jul; 21(4):292-7.
5. Matoso A, et al. Comparison of thyroid transcription factor-1 expression by 2 monoclonal antibodies in pulmonary and nonpulmonary primary tumors. Appl Immunohistochem Mol Morphol. 2010 Mar; 18(2):142-9.
6. Ordóñez NG. Value of thyroid transcription factor-1 immunostaining in tumor diagnosis: a review and update. Appl Immunohistochem Mol Morphol. 2012 Oct; 20 (5):429-44.